Questões de Vestibular
Sobre interpretação de texto | reading comprehension em inglês
Foram encontradas 5.299 questões
Read the text below and answer the question.
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
Read the text below and answer the question.
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
Read the text below and answer the question.
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
Read the text below and answer the question.
Advancing gender equity in medicine
[…]
The problem of gender inequity in medical leadership is not the result of too few candidates who are not men with the appropriate experience and training to fulfill leadership roles, nor can it be explained by merely suggesting that different genders do not have the same aspirations as men. Gender inequity is largely underpinned by socially constructed gender norms, roles and relations. For example, gender roles explain why female clinicians with children spend 100.2 minutes more per day on household activities and child care than their male counterparts. This makes it more challenging for female clinicians with children to get ahead. Gender norms explain why more men are given leadership opportunities and have stronger letters of reference than other genders. Furthermore, gender relations explain why men have fewer consequences for uncivil behaviour or for harassment in the workplace compared with other genders. A recent observational study of operating room culture evaluated the prevalence and predictors of exposure to disruptive behaviour in the operating room. Disruptive behaviour was described as a range of unacceptable workplace behaviours, including incivility, bullying and harassment. A further definition provided is “interpersonal behaviour (i.e., directed toward others or occurring in the presence of others) that results in a perceived threat to victims and/or witnesses and violates a reasonable person’s standard of respectful behaviour.” The study found that clinicians who are women report more exposure to disruptive behaviour and are substantially less confident or empowered to take action to address incivility in their hospital and university settings. Gender and sexual harassment may be associated with environments that exhibit gender inequity in pay, opportunity and promotion. Disruptive behaviour and overt harassment likely endure within our medical institutions because the offenders are often considered invaluable to the organization for their stature, leadership, productivity or reputation, and are largely not held unaccountable for their actions, which further amplifies gender inequities.
Ensuring gender equity in medicine is an issue of justice and rights. Having more physicians who are women and more women in health policy leadership also appears to enhance the provision of high-quality patient care. Large, well-conducted observational studies have shown that patients of female clinicians experience better quality of care for diabetes, and significantly lower rates of mortality, hospital readmissions and emergency department visits than those treated by male clinicians. One study considered that reasons for this may include that women spend more time with their patients, are more patient-centred in their approach and provide more evidence-based care. Two recent opinion pieces discuss research showing that female representation on corporate boards, such as hospital boards, results in more socially thoughtful decisions and less corruption. Without gender equity, we risk extinguishing creative solutions to complex health problems and, most importantly, limiting patient access to the best care.
From: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8034331/ CMAJ. 2021 Feb 16; 193(7): E244–E250.
Based on the text, mark the statements below as true (T) or false (F).
( ) Gender inequity in medical leadership is due to few women who want to take leading positions.
( ) Difference between genders has little effect when disciplining transgressive attitudes at work.
( ) Women physicians have been found to improve the quality of health care services.
The statements are, respectively,
Read the advertisement.
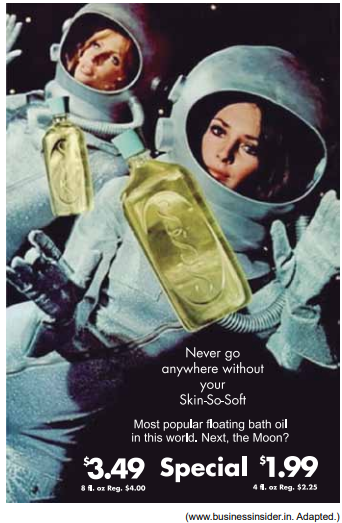
The advertisement uses text and the image of two women astronauts in spacesuits to suggest that both the bath oil “Skin-So-Soft” and the suit

Online Education and Its Effective Practice: A Research Review
By: Anna Sun, Xiufang Chen
Online education is here to stay and grow. The review of its history clearly shows that online education has developed rapidly, mostly as a result of Internet connectivity, advanced technology, and a massive market. It has evolved from 19th century correspondence programs to the 21st century’s vibrant and well-designed institutional online courses.
The fast development of the Internet and the World Wide Web (WWW) has produced numerous benefits to education. Online education provides potential opportunities to open new markets for higher education institutions. Many adult learners may enjoy the flexibility when they have to balance work, study, and family responsibilities. The wide range of various technology advancements used by universities’ online programs may promote the interaction between students and instructors, and among students at large. Finally, the upgraded technology and software may allow instructors, students, and university administrators to collect data, feedback, and evaluation regarding their online experiences.
We can anticipate that online education will continue to increase its presence and influence higher education through a vigorous process of reshaping, refining, and restructuring. It is unlikely, however, to replace entirely traditional higher education, but merely to be an alternative. But, because of its flexibility and accessibility, online education is gaining in popularity, especially for people who are otherwise unable to obtain education because of physical distance, schedule conflicts, and unaffordable costs.
Available in: https://www.informingscience.org/
Publications/3502. Access 28 set. 2022. Adapted
Online Education and Its Effective Practice: A Research Review
By: Anna Sun, Xiufang Chen
Online education is here to stay and grow. The review of its history clearly shows that online education has developed rapidly, mostly as a result of Internet connectivity, advanced technology, and a massive market. It has evolved from 19th century correspondence programs to the 21st century’s vibrant and well-designed institutional online courses.
The fast development of the Internet and the World Wide Web (WWW) has produced numerous benefits to education. Online education provides potential opportunities to open new markets for higher education institutions. Many adult learners may enjoy the flexibility when they have to balance work, study, and family responsibilities. The wide range of various technology advancements used by universities’ online programs may promote the interaction between students and instructors, and among students at large. Finally, the upgraded technology and software may allow instructors, students, and university administrators to collect data, feedback, and evaluation regarding their online experiences.
We can anticipate that online education will continue to increase its presence and influence higher education through a vigorous process of reshaping, refining, and restructuring. It is unlikely, however, to replace entirely traditional higher education, but merely to be an alternative. But, because of its flexibility and accessibility, online education is gaining in popularity, especially for people who are otherwise unable to obtain education because of physical distance, schedule conflicts, and unaffordable costs.
Available in: https://www.informingscience.org/
Publications/3502. Access 28 set. 2022. Adapted
Online Education and Its Effective Practice: A Research Review
By: Anna Sun, Xiufang Chen
Online education is here to stay and grow. The review of its history clearly shows that online education has developed rapidly, mostly as a result of Internet connectivity, advanced technology, and a massive market. It has evolved from 19th century correspondence programs to the 21st century’s vibrant and well-designed institutional online courses.
The fast development of the Internet and the World Wide Web (WWW) has produced numerous benefits to education. Online education provides potential opportunities to open new markets for higher education institutions. Many adult learners may enjoy the flexibility when they have to balance work, study, and family responsibilities. The wide range of various technology advancements used by universities’ online programs may promote the interaction between students and instructors, and among students at large. Finally, the upgraded technology and software may allow instructors, students, and university administrators to collect data, feedback, and evaluation regarding their online experiences.
We can anticipate that online education will continue to increase its presence and influence higher education through a vigorous process of reshaping, refining, and restructuring. It is unlikely, however, to replace entirely traditional higher education, but merely to be an alternative. But, because of its flexibility and accessibility, online education is gaining in popularity, especially for people who are otherwise unable to obtain education because of physical distance, schedule conflicts, and unaffordable costs.
Available in: https://www.informingscience.org/
Publications/3502. Access 28 set. 2022. Adapted

Available in: https://www.lingq.com/blog/english-language-memes/. Access in: 20 nov. 2021
Com base na imagem apresentada, é correto afirmar que