Questões de Vestibular
Nível médio
Foram encontradas 71.618 questões
Resolva questões gratuitamente!
Junte-se a mais de 4 milhões de concurseiros!
Ano: 2018
Banca:
VUNESP
Órgão:
UEA
Prova:
VUNESP - 2018 - UEA - 004. Prova de Conhecimentos Específicos - Exatas |
Q1801639
Matemática
Os gráficos das funções f(x) = –x2
+ 5 e g(x) = –2x + 5 estão
representados em um sistema de coordenadas cartesianas
ortogonais. Os pontos V e P são comuns aos dois gráficos,
pertencendo V ao eixo das ordenadas, conforme mostra a
figura.
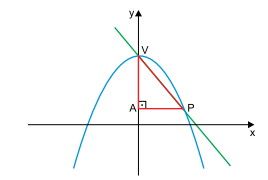
Nessas condições, o perímetro do triângulo retângulo VAP indicado na figura é igual a
Nessas condições, o perímetro do triângulo retângulo VAP indicado na figura é igual a
Ano: 2018
Banca:
VUNESP
Órgão:
UEA
Prova:
VUNESP - 2018 - UEA - 004. Prova de Conhecimentos Específicos - Exatas |
Q1801638
Matemática
Uma das raízes da equação polinomial
x3
+ (k + 1)x2
+ (k + 9)x + 9 = 0 é x1
= –1. As outras duas
raízes são iguais. A soma das três raízes, para k > 0, é igual a
Ano: 2018
Banca:
VUNESP
Órgão:
UEA
Prova:
VUNESP - 2018 - UEA - 004. Prova de Conhecimentos Específicos - Exatas |
Q1801637
Matemática
Deseja-se formar uma comissão composta de três membros.
Sabendo-se que as escolhas devem ser feitas dentre um grupo de 10 pessoas, o número de diferentes comissões que
poderão ser formadas é igual a
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799006
Física
A figura representa um circuito elétrico de lâmpadas utilizadas na decoração de árvores de natal.
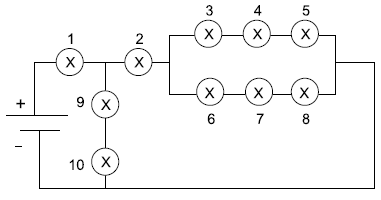
Se na lâmpada 6 for instalado um dispositivo de pisca-pisca, quando ela se apagar, certamente se apagarão as lâmpadas
Se na lâmpada 6 for instalado um dispositivo de pisca-pisca, quando ela se apagar, certamente se apagarão as lâmpadas
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799005
Física
Em uma aula de laboratório, os alunos devem montar um circuito simples para que uma lâmpada (X) possa ser acesa por
meio da ligação em série com uma pilha considerada ideal.
Se nesse circuito forem incluídas as ligações de um voltímetro (V) e de um amperímetro (A), o circuito a ser montado
deve ser:
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799004
Física
A experiência realizada com o tubo de Crookes foi importante
para a descoberta do elétron. Quando duas placas metálicas eletrizadas foram acopladas, uma positivamente e outra
negativamente, desviaram os raios luminosos emitidos por
qualquer gás colocado no interior do tubo, atraído pela placa
positiva e repelido pela negativa.
A figura representa o tubo de Crookes, no qual há dois pares de placas, sendo um par disposto horizontalmente (P1, P2) e o outro par, disposto verticalmente (P3, P4).
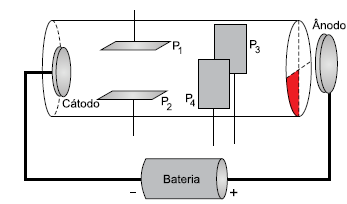
Para que o raio luminoso emitido pelo gás ilumine a parte vermelha do tubo, as placas P1, P2, P3 e P4 devem estar eletrizadas, respectivamente, com cargas de sinais
A figura representa o tubo de Crookes, no qual há dois pares de placas, sendo um par disposto horizontalmente (P1, P2) e o outro par, disposto verticalmente (P3, P4).
Para que o raio luminoso emitido pelo gás ilumine a parte vermelha do tubo, as placas P1, P2, P3 e P4 devem estar eletrizadas, respectivamente, com cargas de sinais
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799003
Física
A figura representa um tanque cheio de água sobre cuja superfície se propaga uma onda de amplitude A e comprimento
de onda λ. Quando essa onda passa por um obstáculo de
duas fendas (1 e 2) ocorrem dois fenômenos (F1
e F2).
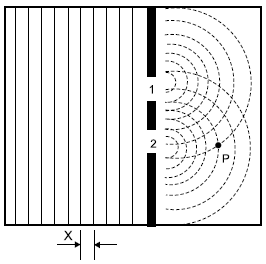
A denominação dos fenômenos F1 e F2, a grandeza indicada em X e o valor da amplitude da onda em P são, respectivamente,
A denominação dos fenômenos F1 e F2, a grandeza indicada em X e o valor da amplitude da onda em P são, respectivamente,
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799002
Física
Uma lupa converge os raios solares a uma distância de
20 cm do centro óptico da lente. Nessa situação, a distância
focal da lente é igual a
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799001
Física
Três recipientes, A, B e C, de mesmo volume e hermeticamente fechados, contêm gases ideais. A massa total do gás e
a velocidade média das moléculas contidas em cada um dos
recipientes estão indicadas na tabela.
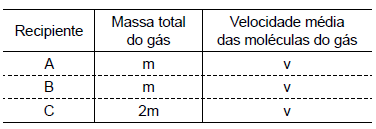
Sabendo-se que a temperatura de um gás ideal é diretamente proporcional à energia cinética média de suas moléculas, a relação entre as temperaturas TA, TB e TC é
Sabendo-se que a temperatura de um gás ideal é diretamente proporcional à energia cinética média de suas moléculas, a relação entre as temperaturas TA, TB e TC é
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1799000
Física
Uma escala termométrica R foi criada para uso em laboratório. Nela, o valor de 0 °R equivale à temperatura de –20 °C e
o valor de 100 °R equivale à temperatura de 40 °C.
Nessa escala, a temperatura de 66 °R, corresponde à temperatura de
Nessa escala, a temperatura de 66 °R, corresponde à temperatura de
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798999
Física
A figura ilustra a experiência de Torricelli, realizada para
medir a pressão atmosférica, utilizando um tubo cheio de
mercúrio e comparando a pressão nos pontos B e C.
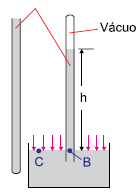
Considere que o tubo da experiência esteja preenchido por um líquido de densidade desconhecida, que a altura h seja 50 cm, que a aceleração da gravidade seja 10m/s2 e que a pressão atmosférica local seja 1 × 105 Pa. A densidade desse líquido dentro do tubo é de
Considere que o tubo da experiência esteja preenchido por um líquido de densidade desconhecida, que a altura h seja 50 cm, que a aceleração da gravidade seja 10m/s2 e que a pressão atmosférica local seja 1 × 105 Pa. A densidade desse líquido dentro do tubo é de
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798998
Física
Do alto de uma escada (ponto A) um bloco, de dimensão desprezível e massa igual a 1 kg, foi solto sobre um aparelho de
ginástica conhecido como jump (uma pequena cama elástica). Esse aparelho, apoiado na altura da linha de referência,
pode ser considerado uma mola ideal de constante elástica
igual a 7600 N/m. Quando ele não está deformado, possui
altura igual a 30 cm.
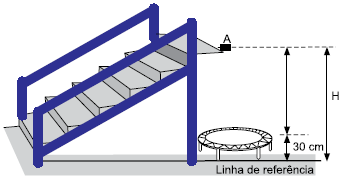
Considere que a deformação causada pelo bloco ao cair sobre o jump foi de 10 cm e que a aceleração da gravidade local seja 10 m/s². Nessas condições, a altura H, em relação à linha de referência, é de
Considere que a deformação causada pelo bloco ao cair sobre o jump foi de 10 cm e que a aceleração da gravidade local seja 10 m/s². Nessas condições, a altura H, em relação à linha de referência, é de
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798997
Física
Um carro de competição percorre metade de um circuito
com velocidade média de 200 km/h. Na segunda metade do
circuito, o desempenho do carro melhora e sua velocidade
média passa a ser 300 km/h. A velocidade média desse carro
quando ele completa todo o circuito é de
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798996
Inglês
Texto associado

Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
Assinale a alternativa cujo trecho evidencia a posição atual
da autora sobre o desafio apresentado no título.
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798995
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No trecho do sétimo parágrafo “However, there’s also a lot of
misleading information, and information that’s simply untrue”,
o termo sublinhado pode ser substituído, sem alteração de
sentido, por
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798994
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
De acordo com o quinto e o sexto parágrafos, um dos benefícios dos dados médicos disponíveis na internet é
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798993
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No trecho do quinto parágrafo “as there is in thinking the
expertise of all people is equivalent”, o termo sublinhado equivale, em português, a
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798992
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
De acordo com o quarto parágrafo, a profissão médica contribui para que as pessoas recorram à internet em vez de
recorrer a médicos. A justificativa apresentada é que
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798991
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No trecho do quarto parágrafo “the information we do like is
most credible, regardless of its source”, a expressão sublinhada equivale, em português, a
Ano: 2018
Banca:
VUNESP
Órgão:
SÃO CAMILO
Prova:
VUNESP - 2018 - SÃO CAMILO - Processo Seletivo - 2º Semestre de 2018 - Medicina |
Q1798990
Inglês
Texto associado
Leia o texto para responder à questão.
The challenge of doctor-patient relations in the internet age
“Let me do some research and I’ll get back to you,” my
patient said. My patient, a 19-year-old student, had already
taken time off from school because of her anxiety. I was her
psychiatrist, with over two decades of experience treating
university students, and had just explained my diagnostic
impressions based on a lengthy evaluation. I’d recommended
that she try a medicine I expected would help. I’d also laid out
the risks and benefits of other treatment options.
“Do you have additional questions I can answer?” I asked.
I wanted to let her know that’s why I was there, to cull the
research, to help make sense of it. “No, I like to go online and
look for myself,” she said.
More and more, I see students turning away from the
expertise that a live person can offer and instead turning to
the vast and somehow more objective-seeming “expertise” of
the digital world.
In an age when journalism we don’t like can be dismissed
as “fake news,” suggesting that the information we do like
is most credible, regardless of its source, it’s not hard to
understand why young people do this. The medical profession
itself, under managed care, has played a role as well, providing
less time for doctor-patient interactions and undermining the
chances that a personal relationship and trust can develop.
Under the guise of efficiency, medical test results are now
often released directly to patients, sometimes before or even
without the benefit of any interpretation.
But there’s danger in trusting data over people, as there
is in thinking the expertise of all people is equivalent. When
it comes to health, digital natives may not be learning how to
navigate effectively. And the consequences could be harmful.
The availability of health data on the internet has its
benefits. Online, for example, we can find explanations and
solutions for symptoms we might be too embarrassed, or
afraid, to discuss with another person, in person. Or, for lifethreatening diseases, we can locate clinical trials our doctors
may not be aware of.
However, there’s also a lot of misleading information, and
information that’s simply untrue. The internet is full of people
selling things – supplements, treatment regimens that have
not been rigorously tested, even prescription medications –
and making false promises that have not been scrutinized
by regulatory agencies. Sometimes, as in the case of some
websites that promote “an anorexic diet” for “aggressive”
weight loss, the information can encourage life-threatening
behavior.
Years ago, when we discussed paternalism versus patient
autonomy in my medical school ethics class, I came down
strongly in favor of autonomy. Who but the patient could best
decide what was right for him or her? But years of clinical –
and personal – experience have taught me that information
in and of itself is insufficient. Judgment is also indispensable,
especially in complex situations, and the capacity for good
judgment rests within people, not data sets.
(Doris Iarovici is a psychiatrist at Harvard University’s Counseling and
Mental Health Services and the author of Mental Health Issues and the
University Student. www.nytimes.com, 01.03.2018. Adaptado.)
No terceiro parágrafo, o termo “expertise” está entre aspas
para